


From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
+ General Considerations
- Brain tumors occur in cats with an incidence of 0.0035% overall and account for 2.2% of all tumors
- Primary tumors accounted for 70.6% of feline brain tumors, LSA for 14.4%, metastatic tumors 5.6%, and direct extension from extracranial sites for 3.8% of feline brain tumors
- 7.5% cats have ≥ 2 tumors of the same type and 10% cats have 2 different types of tumors
- Sex predisposition: males
- Lesion location was predictive of tumor type:
- LSA have diffuse cerebral or brainstem involvement
- Meningiomas involve the 3rd ventricle
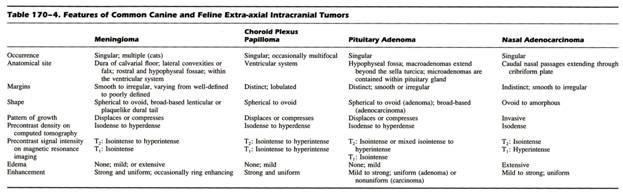
+ Meningioma
- Meningioma is the most common primary brain tumor in cats (56%-69%)
- Meningiomas are extra-axial and supratentorial tumors arising from the dura mater, pia mater, or subarachnoid
- Meningiomas attachment to the dura or leptomeninges may be broad (= sessile), narrow (= pedunculated), or total (= meningioma en plaque)
- Meningioma can involve multiple intracranial sites (14%-17%)
- Meningiomas are commonly located rostral to the tentorium, over the cerebral convexities, and in the 3rd ventricle
- Meningioma is reported more frequently in young cats with mucopolysaccharidiosis type I
- Feline meningiomas are benign and expansile
- Meningiomas are classified as meningoepithelial, fibroblastic, transitional, psammomatous, angioblastic, papillary, granular cell, myxoid, and anaplastic, with most meningoepithelial or psammomatous in cats
+ Other Brain Tumors
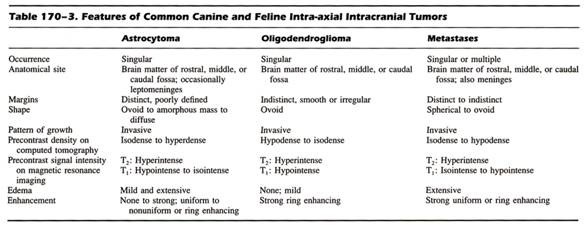
- Other primary brain tumors include LSA (primary or secondary, 14%), pituitary tumor (9%), gliomas (i.e., astrocytoma, and oligodendroglioma, 8%), ependymoma, choroid plexus papilloma, medulloblastoma, olfactory neuroblastoma, and gangliocytoma
- LSA is secondary to multicentric LSA in 71% cats and associated with FeLV infection in 18% cats
- Pituitary tumors are extra-axial and supratentorial tumors
- Glioma and oligodendroglioma are intra-axial and supratentorial tumors
- Neuroepithelial tumors (i.e., ependymoma) are supratentorial and involve either the 3rd ventricle or lateral ventricle
- Secondary tumors affecting the brain include:
- Local extension from nasal tumors, pituitary tumors, middle ear tumors, and skull tumors
- Metastatic brain tumors include mammary, prostatic or pulmonary ADC, HSA, and ovarian dysgerminoma
PATHOPHYSIOLOGY
Primary Brain Tumors
+ General Considerations
- Intracranial tumors are classified as primary or secondary
- Primary brain tumors arise from cells normally found in brain and meninges including neuroepithelium, lymphoid tissue, germ cells, endothelial cells, and malformed tissue
+ Benign versus Malignant
- Cytologic classification of malignancy: anaplasia (i.e., cytoplasmic and nuclear pleomorphism), cellularity, necrosis, mitosis, and invasiveness
- Biologic malignancy will cause death
- Majority of cytologically malignant tumors will also be biologically malignant
- Benign tumors can also be biologically malignant due to secondary effects such as increased intracranial pressure
- Feline meningioma is well-defined with clear demarcation between tumor and abnormal tissue
+ Clinical Effects
- Primary brain tumors can cause clinical signs through primary and secondary effects
- Primary effects of primary brain tumors include:
- Infiltration of nervous tissue
- Compression of adjacent anatomic structures
- Disruption of cerebral vasculature
- Local necrosis
- Secondary effects of primary brain tumors include:
- Disturbed CSF flow resulting in hydrocephalus
- Increased intracranial pressure
- Cerebral edema
- Brain herniation
- Secondary effects are usually more diffuse or generalized and may mask location of focal intracranial lesion
- primary brain tumors are usually slow growing allowing adjacent structures to adapt to gradual increase in pressure with minimal and vague clinical signs (i.e., subtle behavioural changes)
- rapid progression of clinical signs can be caused by overwhelming of compensatory mechanisms
- rapidly growing tumors will result in an acute onset of clinical signs with no premonitory signs due to poor ability of compensatory mechanisms to adapt to rapid tumor growth
+ Invasion by Primary Brain Tumors
- Primary brain tumors have a distinct pattern of spread due to lack of lymphatic channels
- Major patterns include local invasion and CSF seeding
- Primary brain tumors (i.e., astrocytoma) contain cells which are able to invade normal brain
- Seeding may occur by spread along brain surface to local sites or through CSF to spinal subarachnoid space and distant sites (= drop metastases)
- Hematogenous spread is possible, but extracranial metastasis is rare
+ Secondary Brain Tumors
Due to either hematogenous metastasis or local invasion or extension
CLINICAL signs
+ General Considerations
Nature and course of neurologic signs depends on location, extent and rate of growth
+ Premonitory Signs
- Vague signs are common due to slow growth of primary brain tumors
- Vague signs are often overlooked until brain dysfunction is well developed
- Vague signs may be manifestation of headache (common in humans) and include decreased purring and reduced activity levels
+ Clinical Signs
- Seizures (focal or generalized) are the most common clinical sign in cats and dogs with primary brain tumors
- Seizures are commonly associated with tumors of the frontal lobe (44%), olfactory region (20%), parietal lobes (20%), and extension of nasal ADC (11%)
- Other clinical signs include circling (23%), ataxia (21%), ataxia, and cervical spinal hyperesthesia
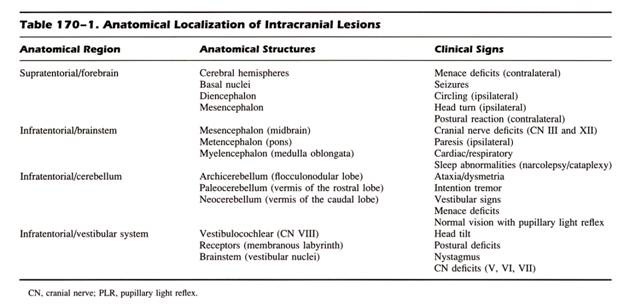
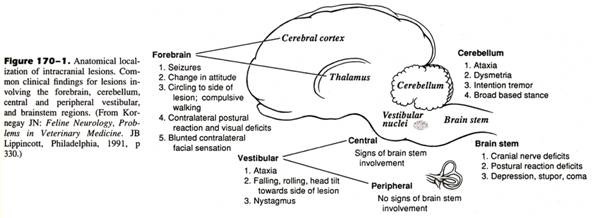
+ Neurologic Signs
 From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
- Brain stem tumors cause cranial nerve deficits
- Frontoparietal tumors cause seizures, behavioural changes, circling, head pressing, visual deficits, proprioceptive deficits with normal to near-normal gait, hemi-inattention syndrome (= hemi-neglect syndrome), and spinal hyperesthesia
- Hemi-inattention syndrome: ignore environmental stimuli on contralateral side to tumor
- Optic nerve or occipital lobe tumors result in visual deficits
- Cerebromedullary, brain stem, and temporal lobe lesions can cause hearing loss
- Cribriform plate, olfactory bulb and peduncle, and piriform or temporal lobe tumors cause problems with smelling
- Cerebellar and vestibular tumors will cause ataxia, dysmetria, intention tremors, and menace deficits with normal vision
 From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
+ Secondary Neurologic Signs
- Secondary effects of brain tumors represent either a large tumor or significant cerebral edema
- Secondary neurologic signs include alterations in behaviour, circling, head pressing, compulsive walking, altered states of consciousness, and associated locomotor disturbances
- Majority of animals with primary brain tumors will present for either seizures or secondary neurologic signs
DIAGNOSIS
+ General Considerations
- History, clinical signs, and physical and neurologic examination
- Minimum data base: hematology, serum biochemistry, urinalysis, thoracic radiographs, and abdominal ultrasound to exclude extracranial causes of cerebral dysfunction
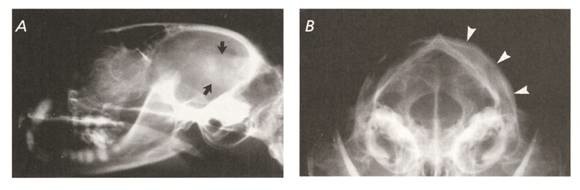
+ Survey Skull Radiographs
- Survey skull radiographs have limited value except for skull and nasal tumors
- Hyperostosis of the overlying calvarium is reported in up to 73% of feline meningiomas
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
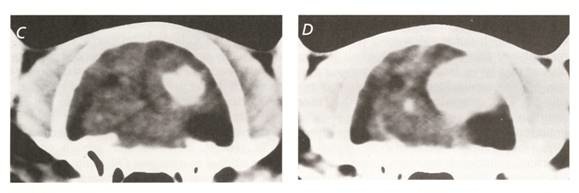
Advanced Imaging
+ General Considerations
- Advanced imaging techniques include ventriculography, cerebral angiography, cavernous sinus venography, cisternography, and scintigraphy
- However, these techniques have been superceded by CT and MRI as they do not provide information on the extent of tumor involvement and relationship to adjacent structures
- MRI is superior to CT in detecting many features associated with brain tumors such as edema, cyst formation, changes in vascularity, hemorrhage, and necrosis
- Primary brain tumors may have characteristic CT or MRI features, but these are not pathognomonic
+ Magnetic Resonance Imaging Appearance
- Majority of tumors are round or oval, except plaque-like tumors are always meningiomas
- Majority of tumors are hyperintense and heterogenous on T2-weighted images
- Majority of tumors are hypo- or isointense and heterogenous or homogenous on T1-weighted images
- Majority of tumors show marked contrast enhancement
- Ring enhancement is seen predominantly in gliomas, but also observed in meningiomas and pituitary tumors
+ Tumor Location
- Extra-axial tumors include meningioma, LSA, pituitary tumor, olfactory neuroblastoma, ventricular tumors (i.e., choroid plexus tumor and ependymoma), and direct extension of nasal tumors
- Meningioma accounts for 83% of extra-axial lesions
- Extra-axial tumors affecting the frontal lobe can be difficult to predict based on axial location alone as 55% are meningiomas, 20 LSA, 15% nasal tumors, and 10% olfactory neuroblastomas
- However, meningiomas and LSA do not cause cribriform plate destruction, whereas both tumors extending from the nasal cavity and olfactory neuroblastomas cause cribriform plate destruction
+ Meningiomas
- MRI appearance of feline meningiomas include:
- Extra-axial location
- Ovoid to round in shape with distinct margins
- Hyperintense and heterogenous on T2-weighted images
- Hypo- or isointense on T1-weight images
- Intense contrast enhancement
- Mass effect (97%) with a broad base (49%) and dural tail sign (64%)
- Other findings included lateral ventricular enlargement (64%), transtentorial herniation (42%), cerebellar herniation (21%) ± mineralization
 From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
 From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
 From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
From: Slatter DH (ed): Textbook of Small Animal Surgery (3rd ed).
+ Cerebrospinal Fluid Analysis
- CSF analysis will assist in excluding inflammatory causes of neurologic disease and may aid in diagnosis of primary brain tumor
- CSF collection can result in brain herniation due to shift in intracranial pressure
- CSF collection is recommended after advanced imaging
- CSF changes include increased protein content and normal to increased white cell count
- Typical CSF changes observed in < 40% of dogs with primary brain tumors with 50% having non-specific changes and 10% with normal CSF
- Neoplastic cells can occasionally be detected in CSF following sedimentation techniques
Biopsy
+ General Considerations
- Only method to provide a definitive diagnosis prior to therapy
- Not commonly performed due to practical considerations such as cost and morbidity
- Techniques include ultrasound-guided biopsy, freehand CT-guided biopsy, and CT-guided stereotactic brain biopsy
+ Other Diagnostic Techniques
Lipid-associated sialoprotein in CSF is a marker used in humans which is diagnostic for presence of intracranial malignancy and can be used to assess response to therapy
Treatment
+ General Considerations
- Aims of treatment for brain tumors include:
- Tumor removal or cytoreduction
- Control secondary effects (i.e., increased intracranial pressure and cerebral edema)
- Treatment options include conservative or palliative management, surgery, radiation therapy, chemotherapy and immunotherapy
- Gene therapy is promising but currently a research tool
+ Palliative Management
- Corticosteroids can be used to reduce edema associated with brain tumors and retard tumor growth if LSA is suspected with dramatic improvement in clinical signs which can be sustained for weeks to months
- Phenobarbitone and potassium bromide can be used to control seizure activity
+ Surgical Management
- Surgical management of brain tumors is more common with advanced imaging providing accurate information on location, size, extent and invasiveness of tumor, and improved knowledge in anesthetic, surgical, and critical care
- Complete excision is determined by location, size, extent, invasiveness, and tumor type
- Complete excision is more likely with:
- Meningiomas (especially cats)
- Tumors over cerebral convexities and frontal lobes
- Complete resection of canine meningiomas is difficult because they are friable, lack demarcation from normal brain tissue, and can be infiltrative
- Morbidity and mortality is high for tumors of the caudal fossa and brain stem
- Partial resection can provide a histologic diagnosis and decrease clinical signs associated with the tumor resulting in a better candidate for adjunctive radiation therapy
- Radical cerebral cortical resection (i.e., frontal and parietotemporal lobectomy) is well tolerated in normal dogs with unilateral orbicularis oculi paralysis common and central amaurosis following parietotemporal lobectomy
- Tumor seeding is possible with cytoreductive surgery
- Complications: neurologic deterioration, seizures, pneumonia, and tension pneumocephalus
Radiation Therapy
+ General Considerations
- Radiation therapy can be used either alone or in combination with other therapies such as surgery or chemotherapy
- Radiation therapy is recommended for treatment of pituitary tumors, LSA, and secondary brain tumors
- Aim: destroy tumor tissue while minimizing damage to normal cerebral tissue
- Orthovoltage radiation therapy has been used but is not ideal due to poor penetration and limited field configuration
- External beam megavoltage radiation therapy is preferred as, with CT and MRI imaging, treatment planning is superior with resultant decrease damage to normal tissue
+ Protocols
- Fractionated protocols of 2.7-3.0 Gy over 3-5 weeks provides good results with minimal adverse affects
- Other techniques include:
- Hypofractionated protocols with 5 weekly fractions for 34 Gy total dose
- Super-fractionation with ≥ 2 fractions per day
- Fractionated radiation therapy combined with hyperthermia or radiation sensitizers
- Boron neutron capture therapy
- Brachytherapy (limited success in dogs)
- CT-guided stereotactic radiosurgery with application of highly localized single fraction of radiation
+ Complications
- Tissue tolerance for whole brain is 48 Gy but localized tissue tolerance is 54 Gy
- Adverse effects are usually late and delayed and include brain necrosis
- Delayed radiation effects responsible for up to 14% (12/83) mortality rate
+ Chemotherapy
Chemotherapy is not frequently used for primary brain tumors due to:
- Blood-brain barrier
- Tumor heterogeneity may result in only certain cell populations sensitive to chemotherapeutic drugs
- Brain tumors may only be sensitive at doses which are toxic to normal brain and other tissues
- Options include intra-arterial delivery, high-dose systemic therapy, liposome-encapsulated therapy, and blood-brain barrier disruption (i.e., osmotic disruption or transient disruption with bradykinin analogues)
- LSA, medulloblastoma, and oligodendroglioma are very chemotherapy sensitive brain tumors
- Intrathecal cytosine arabinoside has been used for CNS LSA because of good blood-brain barrier penetrations
- Carmustine and lomustine (CCNU) have resulted in significant reduction in tumor size and improvement in neurologic signs in dogs with glial cell tumors
PROGNOSIS
+ General Considerations
- Female sex hormone concentration correlates with growth and biologic behaviour of meningioma
- Functional importance of progesterone receptors and their modulation is unknown
+ Untreated Primary Brain Tumors
Mean ST for untreated meningioma: 18 days in cats
Treated Primary Brain Tumors
+ General Considerations
- Prognosis is improved with interventional therapy: surgery, radiation therapy, chemotherapy, or immunotherapy
Poor prognostic factors include:
- Moderate to severe neurologic signs
- Rapid and progressive clinical course
- Increased CSF white cell count
- Involvement of multiple brain regions
- Primary brain tumor other than meningioma and secondary brain tumors
- Low postoperative PCV and survival in cats with meningiomas
+ Surgery
- MST for intracranial meningioma in cats is 485-810 days
- 6-month survival rate 71%, 12-month survival rate 66%, and 2-year survival rate 50%
- 21% local tumor recurrence rate with a median DFI 285 days to 27 months
- Prognosis for surgical removal of meningioma in cats and dogs affected by postoperative complications such as infection, cerebral edema, and hemorrhage
+ Other Brain Tumors
- MST for non-meningeal tumors is 414 days, with a 12-month survival rate 40%
- MST for cats with brain LSA treated with prednisone is 21 days
- MST for cats with pituitary tumors is 52.5 days
- Survival times for cats with gliomas range from 1-179 days
- Survival times for cats with oligodendroglioma range from 1-30 days
- Survival times for cats with neuroepithelial tumors (i.e., ependymoma) range from 667-685 days in 2 treated cats