Synonyms: multilobular tumor of bone, chondroma rodens, calcifying or juvenile aponeurotic fibroma, cartilage analogue of fibromatosis, and multilobular osteoma, chondroma, or OSA
Multilobular osteochondrosarcoma is an uncommon tumor attributable to abnormal cellular activity arising from the periosteum of bones formed by intramembranous ossification with the cells of origin periosteal cells of the common chondrocranium and viscerocranium, both of which share a common embryonic origin
Multilobular osteochondrosarcoma has a predilection for the skull of dogs with sites including the cranium (i.e., occipital, parietal, and frontal bones), orbit, zygomatic arch, mandible, and maxilla
Other sites includes pelvis, rib, and os penis
Median age 7.5-8.0 years
Median body weight 29 kg
No sex or breed predisposition
Multilobular osteochondrosarcoma has also been diagnosed in other species including the cat, ferret, and horse
+ Clinical Signs
Palpable, fixed, and firm mass
Pain on mouth opening for tumors involving the mandible and zygomatic arch
Exophthalmos
Neurologic abnormalities for tumors involving the cranium
Dyspnea for tumors involving the tympanic bulla
DIAGNOSIS
Imaging
+ Survey Radiographs
Tumor borders are sharply demarcated with limited bone lysis and a course granular mineral density with a lobular pattern (= popcorn appearance with stippled and heavily calcified or ossified regions)
Lack of radiographic evidence of multilobular osteochondrosarcoma has been reported
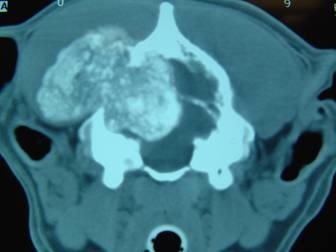
+ Computed Tomography
CT is indicated for detection of tumor calcification, cortical bone and soft tissue involvement, and intramedullary or intracranial extension to aide in surgical planning
Multilobular osteochondrosarcoma has a multilobular appearance with well-defined margins
Multilobular osteochondrosarcoma of the rostral skull and zygomatic arch has a coarse granular appearance
Multilobular osteochondrosarcoma of the caudal skull has a fine granular or stippled appearance
Majority of calvarial multilobular osteochondrosarcoma have significant intracranial involvement
Contrast enhancement is not helpful
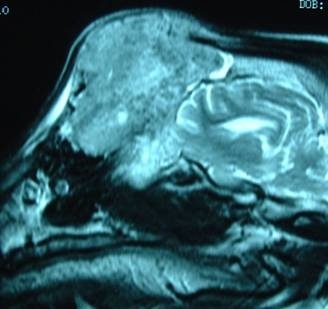
+ Magnetic Resonance Imaging
MRI is indicated for detecting extraosseous and intramedullary extension of skull tumors
T1-weighted images: multilobular osteochondrosarcoma is hypointense compared to the brain, but not CSF, with a rim of contrast enhancement and areas of enhancement interspersed with areas of non-enhancement
T2-weighted images: low signal intensity; enhancement is poor for areas of tumor consisting mainly of osteoid, despite marked vascularity and cellularity, while chondroid forming matrix has intense contrast enhancement
+ Histology
Histologic features: multiple lobules centered on a core of cartilaginous or bony matrix which is surrounded by a thin layer of spindle cells and separated by fibrovascular septa
Characteristic trilaminar appearance:
Central area of cartilage or bone that may be calcified or ossified
Middle zone of plump, spindle-to-ovoid shaped cells
Peripheral zone of fibrous tissue
Histologic indicators of malignancy include increased mitotic activity, necrosis, hemorrhage, loss of lobular architecture, and overgrowth of 1 of the mesenchymal elements
Histologic grading of multilobular osteochondrosarcoma is prognostic for local tumor recurrence, metastasis, and survival time
TREATMENT
+ Surgical Treatment
Surgical techniques: craniectomy, maxillectomy, mandibulectomy, hemipelvectomy, or rib resection
Cranioplasty, with either allograft of polymethylmethacrylate, has been described
However, infection in prosthetic material can be devastating when used for calvarial reconstruction
Role of chemotherapy and radiation therapy is unknown
Complete response to samarium radiation therapy has been reported in 3 dogs
Pulmonary metastatectomy should be considered for pulmonary metastases due to slow growth rate
Postoperative neurologic recovery can take 1-2 weeks but majority of dogs return to normal
PROGNOSIS
+ Local Recurrence
47%-58% local tumor recurrence rate with median time to local recurrence 426-797 days
Prognostic factors for local recurrence include surgical margins and histologic tumor grade:
Median DFI is significantly increased with complete resection (330 days v > 1,332)
Local tumor recurrence is significantly more likely with grade III multilobular osteochondrosarcoma (78% v 30% for grade I and 47% for grade II tumors)
+ Metastasis
56%-58% metastatic rate with median time to metastasis 426-542 days
Metastatic sites include the lungs (90%), cerebral cortex, pancreas, kidney, mediastinum, and rib
Prognostic factors for metastasis include surgical margins and histologic tumor grade:
Metastasis is significantly more likely with incomplete resection (75% v 25%)
Metastasis is significantly more likely with grade III multilobular osteochondrosarcoma (78% v 30% for grade I and 60% for grade II tumors)
Survival times following detection of pulmonary lesions can be > 12 months
+ Prognosis
MST 24 days for untreated multilobular osteochondrosarcoma
MST 669-797 days for treated multilobular osteochondrosarcoma
Median time to death from recurrent or metastatic disease is 239 days
Prognostic factors: tumor site, histologic grade, and surgical margins
MST for mandibular tumors is significantly better than other sites (1,487 days v 528 days)