

+ General Considerations
- Vaginal and vulval tumors are the 2nd most common canine reproductive tumor and account for 2.4%-3.0% of all canine tumors
- Majority of vaginal and vulval tumors are benign:
- Leiomyoma and fibroma in cat
- Leiomyoma and lipoma in dog
+ Leiomyoma
- 86% of vaginal and vulvar tumors are benign smooth muscle tumors (i.e., leiomyoma and fibroma)
- Majority of leiomyomas arise from vestibule of vulva rather than vagina
- Extraluminal and intraluminal forms have been described:
- Extraluminal present with a slow-growing perineal mass
- Intraluminal are attached to vestibular or vaginal wall by variably sized pedicle and can be multiple
- Mucosa is generally intact but ulceration may occur with exposure and irritation
- Leiomyoma may be hormone dependent:
- Leiomyoma has not been diagnosed in dogs ovariectomized < 2 years
- 15% local tumor recurrence rate in intact and 0% in dogs following ovariohysterectomy
- Mean age 10.8 years
- Breed predisposition: Boxer
- Incidence of leiomyoma higher in nulliparous bitches
- 33% associated with cystic endometrial hyperplasia, ovarian cysts, and mammary gland tumors
+ Lipoma
- Lipoma can arise from perivascular or perivaginal adipose tissue and attach to tuber ischii
- Lipoma can lie within pelvic canal and are usually well-circumscribed and relatively avascular
- Mean age 6.3 years
+ Transmissible Venereal Tumor
- Transmissible venereal tumors occurs in 4-5-year-old dogs with increased risk in free roaming dogs
- Cell origin of transmissible venereal tumors is unknown, but an undifferentiated round cell tumor of reticuloendothelial origin is most likely
- Transmissible venereal tumors have a common origin as chromosomal aberrations are constant and highly specific
- Virus particles have been identified in transmissible venereal tumors
- However, viral etiology is unlikely as the disease cannot be transmitted by cell-free filtrates
- Transmissible venereal tumors are transmitted by contact with genital mucous membranes during coitus
- Transmissible venereal tumors appear as multiple tumors along the mucosal lining of the vagina and vestibule
+ Other
- Benign tumors: sebaceous adenoma, fibrous histiocytoma, benign melanoma, myxoma, and myxofibroma
- Malignant tumors: leiomyosarcoma, ADC, SCC, TCC, HSA, OSA, MCT, and epidermoid carcinoma
- Carcinoma of bladder or urethra may present with palpably enlarged urethral papilla
CLINICAL FEATURES
+ Clinical Signs
- Duration of clinical signs longer for extraluminal compared to intraluminal leiomyoma
- Intraluminal leiomyoma often presents as mass extruding between vulval lips, particularly during estrous
- Other clinical signs include vulval bleeding or discharge, enlarging vulvar mass, dysuria, hematuria, tenesmus, excessive vulval licking, and dystocia
- Lipomas usually present with a slowly growing mass impinging on adjacent structures
+ Diagnosis
- Vaginoscopic examination, retrograde vaginography, and urethrocystography may delineate mass
- Ultrasonography, FNA, and histopathology
Treatment
+ Medical Management
- Local tumor recurrence rate is high for dogs with transmissible venereal tumor and surgery is not recommended
- Transmissible venereal tumors are very response to chemotherapy and radiation therapy
- Chemotherapy: vincristine 0.5-0.7 mg/m 2 IV 4-8 times ± doxorubicin
+ Surgical Management – Benign Tumors
- Exploratory celiotomy for ovariohysterectomy (due to hormonal dependence and local tumor recurrence)
- Conservative surgical resection
- Wide resection probably not required if ovariohysterectomy performed concurrently
- Dorsal episiotomy may be required to provide adequate visualization and ensure complete resection
- Dorsal episiotomy indicated for extraluminal vaginal and vulvar tumors as tumors are usually well-circumscribed and poorly vascularized resulting in good probability of complete excision
- Perineal approach or pubic split is rarely required
+ Surgical Management – Malignant Tumors
- Malignant infiltrative vaginal tumors treated with complete vulvovaginectomy and perineal urethrostomy
- Sternal recumbency in perineal stand with perineum elevated
- Urethra catheterized
- Fusiform skin incision performed around vulva
- Deeper tissues sharply dissected from labia and vestibule
- Constrictor vestibuli and constrictor vulvae muscles are dissected from the vestibule
- Dorsal labial branches of the ventral perineal artery are ligated or bleeding controlled with electrocautery
- Catheterized urethra identified and dissected free from encircling constrictor vestibuli muscles
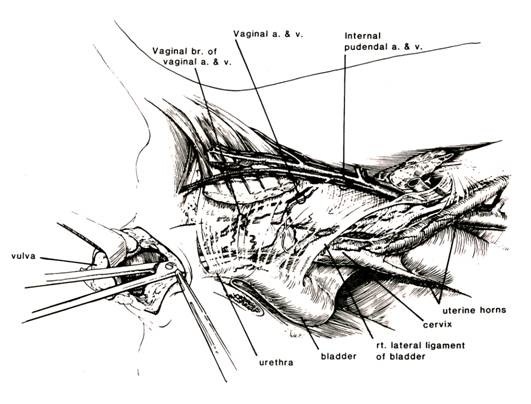 From: Bilbrey SA, et al: Vulvovaginectomy and perineal urethrostomy for neoplasms of the vulva and vagina. Vet Surg 18:450-453, 1989.
From: Bilbrey SA, et al: Vulvovaginectomy and perineal urethrostomy for neoplasms of the vulva and vagina. Vet Surg 18:450-453, 1989.
- Vagina dissected with transection of ischiocavernosus and ischiourethralis muscles
- Dissection continued cranially between paired levator ani muscles to level of cervix
- Vaginal branches of vaginal and uterine arteries and veins ligated
- Vagina transected immediately caudal to cervix in intact bitches or cervix and uterine stump removed in spayed dogs
- Deep tissues closed to reduce dead space
- Perineal urethrostomy performed with transected urethra tractioned caudally, distal end spatulated, and closed in 2 layers with final layer mucosa to skin
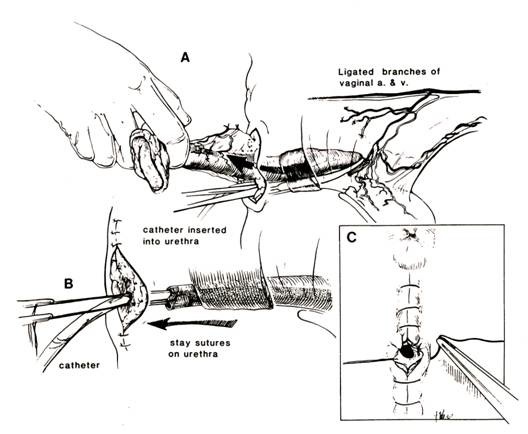 From: Bilbrey SA, et al: Vulvovaginectomy and perineal urethrostomy for neoplasms of the vulva and vagina. Vet Surg 18:450-453, 1989.
From: Bilbrey SA, et al: Vulvovaginectomy and perineal urethrostomy for neoplasms of the vulva and vagina. Vet Surg 18:450-453, 1989.
+ Prognosis
- Complete surgical excision is usually curative
- Guarded to poor prognosis with ADC, TCC, and SCC due to high local tumor recurrence and metastatic rates