CSA is a malignant cartilage-producing neoplasm arising de novo within bone
CSA is the 2nd most common primary bone tumor (5%-10%), but uncommon in the appendicular skeleton
CSA should be differentiated from chondroblastic OSA
Etiology is unknown but can arise at multiple cartilaginous exostoses sites or previous bone lesion
Median age 8.7 years
Breed predisposition: Golden Retriever
61%-91% CSA occur in the axial skeleton (i.e., nasal cavity [26%-36%], ribs, pelvis, vertebrae, and skull)
Other CSA sites include the appendicular skeleton (<20% data-preserve-html-node="true" to 26%), digits, os penis, and extraskeletal sites (i.e., mammary gland, heart valves, aorta, larynx, trachea, lung, and omentum)
CSA is slow to metastasize
Malignant tracheal tumors in dogs include OSA, CSA, MCT, ADC, LSA, and SCC
Benign tracheal tumors in dogs include chondroma, osteochondroma, ecchondroma-osteochondromal dysplasia, extramedullary plasmacytoma, and leiomyoma
Neoplasia of the thyroid gland, esophagus, lung, or aortic chemoreceptor can invade the trachea
Non-neoplastic tracheal masses include polyp, eosinophilic granuloma, nodular amyloidosis, tissue reaction to Filaroides osleri, chondromatous hamartoma, papillomatosis, and hyperplastic tracheitis
Bimodal age distribution with osteochondroma and ecchondroma-osteochondromal dysplasia in dogs < 2 years and other tumor types in dogs > 6 years
Osteochondroma and ecchondroma-osteochondromal dysplasia are benign osseocartilaginous tumors which grow in synchrony with the musculoskeletal system and should stop growing at skeletal maturity
DIAGNOSIS
+ Clinical Signs
Paroxysmal intermittent coughing of several weeks duration
Progressive worsening of dyspnea, stridor, and exercise intolerance
Respiratory signs usually evident when > 50% diameter of airway obstructed
Large masses may be palpable especially in the dog
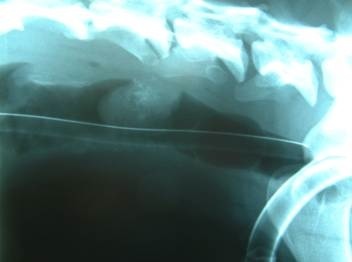
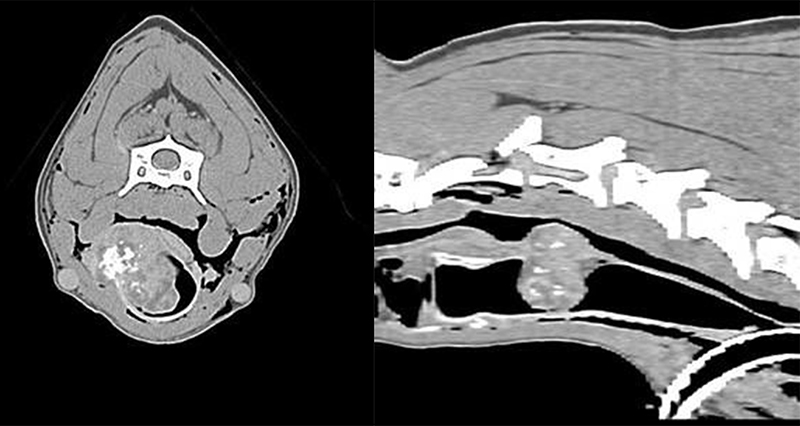
+ Imaging
Survey ± contrast bronchography with survey radiographs usually sufficient due to size of lesions at diagnosis
Other radiographic signs include pulmonary over-expansion, flattening of the diaphragm, and prominent pulmonary vasculature secondary to increased air content in the lower airways
Tracheoscopy provides positive diagnosis with samples collected for brush cytology and histopathology
CT or MRI used in humans
TREATMENT
+ Surgical Resection
Resection and anastomosis
± tracheal wall reconstruction or stenting
+ Other Treatment Options
Radiation therapy
Chemotherapy
Endoscopic removal
Photodynamic therapy
+ Prognosis
Tumor location is prognostic with CSA in the skull, nasal turbinates, and appendicular skeleton having a better prognosis than rib CSA
MST 210-580 days for dogs with nasal CSA and metastasis is very rare
MST 1,080 days for dogs with rib CSA
MST 201-540 days for dogs with appendicular CSA treated with limb amputation ± chemotherapy
12-month survival time 17% and 24-month survival time 13%
Histologic grade: I, II, and III
Histologic grade is an important prognostic indicator for CSA of the same site
Benign tracheal neoplasms have a good prognosis following complete resection
Short-term prognosis is good for dogs with tracheal tumors, but long-term outcome has not been assessed:
Survival times for osteochondroma > 6-8 months
Survival times for ecchondroma-osteochondromal dysplasia > 5-12 months
Survival times for leiomyoma > 6-7 months
Survival times for extramedullary plasmacytoma > 3 months