

Clinical Features
+ Superficial Necrolytic Dermatiti
- glucagonoma is a rare endocrine tumor of the α pancreatic cells and has been reported in 8 dogs
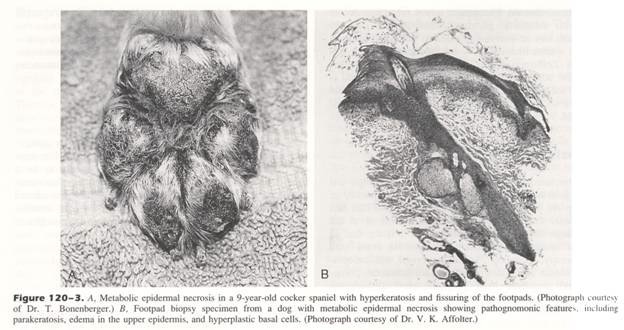
- Glucagonoma is associated with a characteristic dermatitis of the footpads = superficial necrolytic dermatitis
- Synonyms: metabolic epidermal necrosis, necrolytic migratory erythema, and diabetic dermatitis
- Skin lesions can also occur on the muzzle, mucocutaneous junctions, elbow, hocks, pinnae, and external genitalia
- Skin lesions tend to wax and wane and can be pruritic with secondary bacterial infections
- However, superficial necrolytic dermatitis is not pathognomonic for glucagonoma as 78 cases of superficial necrolytic dermatitis have been reported and only 7 of these were diagnosed with concurrent glucagonoma
- Classification scheme has been proposed: superficial necrolytic dermatitis, superficial necrolytic dermatitis and hepatocutaneous syndrome, and suspected superficial necrolytic dermatitis, with glucagonoma reported in:
- 9% of dogs with superficial necrolytic dermatitis
- 60% of dogs with superficial necrolytic dermatitis and hepatocutaneous syndrome
- 31% of dogs with suspected superficial necrolytic dermatitis
- Superficial necrolytic dermatitis resolves following successful surgical resection of the pancreatic glucagonoma
- DDx: pemphigus foliaceus, SLE, generic dog food dermatosis, and zinc-responsive dermatosis
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
+ Diabetes Mellitus
- Glucagon promotes gluconeogenesis and glycogenolysis
- Hyperglycemia will result if there is an excess of glucagon relative to insulin
- Diabetes mellitus will occur if insulin production cannot match the excessive secretion of glucagon
+ Other Clinical Signs
- Other clinical signs include weight loss, polyuria, and polydipsia
- Weight loss is caused by the catabolic effects of glucagon on fat and protein metabolism
+ Diagnosis
- Hematologic and serum biochemical abnormalities include non-regenerative anemia and elevated liver enzymes ± hypoalbuminemia, decreased BUN, and persistent hyperglycemia
- Skin biopsy: diffuse parakeratotic hyperkeratosis with high levels of confluent vacuolation of keratinocytes resulting in epidermal edema, with minimal dermal changes (i.e., perivascular accumulation of lymphocytes and plasma cells)
- Chronic lesions may have superficial to lichenoid inflammatory infiltrates
- Abdominal and thoracic imaging for detection of a pancreatic mass and metastatic disease
- However, pancreatic mass was only detected in 13% (1/8) dogs with ultrasonographic examination
- Multiple diffuse hypoechogenic foci in the liver (= honeycomb pattern) is present in 50% (4/8) dogs with glucagonoma and is consistent with hepatic metastases
- Plasma glucagon levels in the absence of hypoglycemia strongly supports the diagnosis of glucagonoma
+Treatment
- Exploratory celiotomy with partial pancreatectomy and clinical staging for metastatic disease
- Tumor debulking can decrease the intensity of skin lesions in humans with glucagonoma
- Octreotide is recommended for medical management of humans with glucagonoma
- Other medical treatment options include decarbazine and streptozotocin with 5-fluoroucil
+Prognosis
- Prognosis is poor with metastasis common and widespread at diagnosis
- Survival times range from 3 days to 9 months