

+ Etiology
- Tumors of nasal cavity represent approximately 1% of all tumors in dogs
- Etiologic factors include:
- Dolichocephalic breeds
- Dogs living in an urban environment
- Exposure to smoke, indoor kerosene or coal combustion and flea spray
- Sex predisposition in dogs: ± male
- Medium to large sized dogs are more commonly affected
- Median age: 10 years although dogs with sarcomas may present at an earlier ag
+ Pathophysiology
- Nasal tumors are malignant in 80% dogs
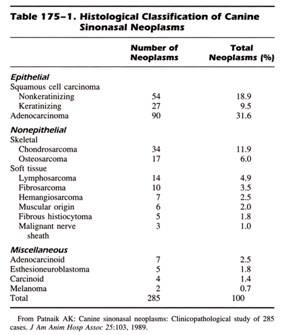
- 60%-75% of malignant tumors in dogs are carcinomas with ADC the most common while others include SCC, undifferentiated carcinoma, TCC, and neuroendocrine tumors
- 25%-40% of malignant tumors are sarcomas such as FSA, CSA, OSA, undifferentiated sarcoma, rhabdomyosarcoma, HSA, leiomyosarcoma, myxosarcoma, and malignant fibrous histiocytoma
- Nasal LSA is rare in both species, but more common in cats and not associated with FeLV infection
- Other round cell tumors include plasmacytoma, transmissible venereal tumor, MCT, and histiocytoma
- Other nasal tumors include malignant melanoma and paranasal meningioma
 From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
- Nasal tumors, regardless of histologic type, are characterized by locally invasive growth
- Metastatic rate is low at diagnosis but reported in up to 50% of dogs at necropsy
- Metastatic sites include lymph nodes and lungs ± bone reported in 2 dogs
- Benign nasal tumors include adenoma, basal cell tumor, fibroma, and neurofibroma
- Nasal vestibule is the most common site for feline nasal SCC, malignant melanoma, and basal cell tumor
DIAGNOSIS
+ General Considerations
- History, clinical signs, survey radiographs, CT, and tissue biopsy
- Hematology and clotting profile to exclude bleeding disorders: platelet count, PCV, ACT, PT, and APTT
- Lymph node aspirates are positive in 10% and thoracic radiographs are usually normal at presentation
- CSF should be collected if CNS involvement: increased CSF pressure, protein, and rarely cell count are abnormal
+ Clinical Signs
- Intermittent and progressive unilateral epistaxis ± mucopurulent discharge
- Other clinical signs: sneezing, reverse sneezing, stertorous respiration, dyspnea, facial deformity, epiphora, and neurologic signs (i.e., seizures, behavioural changes, and obtundation) due to direct invasion of cranial vault
- Mean duration of clinical signs prior to presentation is 3 months
- DDx: bleeding diathesis, hypertension, bacterial or fungal rhinitis, and developmental anomalies
Imaging
+ Survey Radiographs
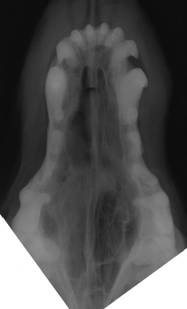
- Nasal radiographs determine extent of disease, presumptive diagnosis, and locate an area for biopsy
- Views: lateral, dorsoventral, frontal sinus, open mouth oblique, and open mouth ventrodorsal
- Radiographic pattern depends on histologic type, duration, and previous treatment
- Mixed pattern of conchal destruction ± increased soft tissue opacity
- Opacification of the ipsilateral frontal sinus is often due to impaired sinus drainage, but extension of the neoplastic process into the frontal sinus can also occur
- Less defined and more destructive appearance with aggressive nasal tumors
- Early neoplasia is difficult to differentiate from rhinitis
- Unilateral increase in nasal opacity with attenuation or obliteration of normal conchal pattern is characteristic of early epithelial nasal neoplasia
- Radiographic appearance becomes more heterogenous due to progressive conchal destruction with tumor progression and growth
- Nasal septum can be deviated or destroyed by neoplastic process, but this is difficult to assess
- Peripheral signs of nasal neoplasia includes soft tissue swelling, facial bone destruction, and periosteal new bone formation, and these signs are usually associated with highly aggressive neoplasms

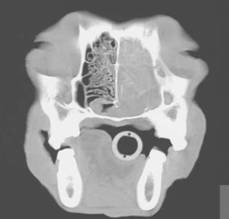
+ Computed Tomography
- CT is preferred for determination of extent of disease and planning for radiation therapy
- Useful for determining extent of disease and involvement of cribriform plate and orbit

+ Biopsy
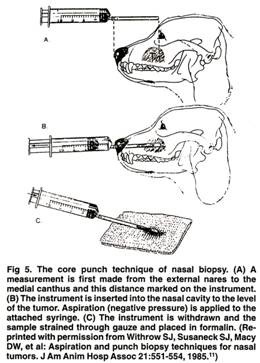
- Trans-nostril technique preferred for core biopsy although rhinoscopic and open techniques also used
- Techniques: punch biopsy, large-bore plastic cannula, curette, or grasping (i.e., melon ball) forceps
- Measure from the external nares to the medial canthus to prevent penetration of cribriform plate
- Mild resistance is usually discernible when tumor tissue is encountered
 From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
- Other techniques: nasal wash with fluid retrieval for cytologic examination (usually unrewarding), brush cytology (often non-diagnostic for mesenchymal tumors), and rhinoscopic biopsy (although samples are small and superficial)
- Complications: mild to moderate hemorrhage
Hemorrhage is usually self-limiting but carotid ligation is occasionally required
Clinical Staging
TREATMENT
+ Surgery
- Palliative
- Nasal neoplasia is usually advanced with bone invasion and critical location adjacent to eyes and brain
- Acute and chronic morbidity with dorsal rhinotomy
- No improvement in survival time with surgery compared to conservative management or surgery and radiation therapy compared to radiation therapy alone
- Principal indication for surgery is rostral nasal tumors (i.e., nasal planum and vestibule)
- Unilateral or bilateral carotid artery ligation may be required to control epistaxis
+ Chemotherapy and Immunotherapy
- No improvement in survival time
- 27% response rate to cisplatin but MST only 20 weeks
- OPLA-cisplatin is a radiation sensitizer and improves survival when used in combination with radiation therapy
+ Photodynamic Therapy
- Photodynamic therapy has been used to treated 1 cat and 3 dogs with nasal tumors using pyropheophorbide-a-hexyl ether as the photosensitizing agent
- Photodynamic therapy is well tolerated with no cutaneous sensitization, but facial swelling is common and resolves within 72 hours
- Clinical signs are controlled for 2 weeks to > 54 weeks
+ External Beam Radiation Therapy
General Considerations
- CT is preferred for planning of radiation field and dosing to limit exposure of normal tissue
- Role of surgical debulking prior to radiation therapy is unknown
- Surgical debulking is required for orthovoltage but optional for cobalt and megavoltage radiation therapy
- Surgical debulking after curative-intent radiation therapy significantly improves survival time
- Dose: 18 fractions at 3 Gy per fraction for 54 Gy total dose
- Accelerated dose: 10 fractions at 4.2 Gy per fraction for 42 Gy total dose
Complications
- Oral mucositis, rhinitis, and radiation-induced moist desquamation for 4-8 weeks
- Treatment of oral mucositis includes tannic acid, glutamine (1.3 g/m 2 q 8 hrs PO), and benzydamine
- Ocular changes (i.e., KCS, corneal ulcers, and cataracts) if eyes included in radiation field and dose > 40 Gy
+ Brachytherapy
- Intracavitary therapy using radioactive isotopes
- Potential problems include dose distribution and radiation exposure to personnel
PROGNOSIS
+ General Considerations
- MST 3-6 months for surgery, chemotherapy, immunotherapy, cryosurgery, and no treatment
- MST 8-23 months for radiation therapy ± surgical debulking, with
- 1-year survival rate 37%-81%
- 2-year survival rate 10%-48%
- MST 580 days for nasal tumors treated with radiation therapy and OPLA-cisplatin (v 325 days in historical group)
- CSA respond better to radiation therapy than other nasal tumors
- ADC responds better to radiation therapy than SCC or undifferentiated carcinomas
- MST 165 days for non-keratinizing nasal SCC
- Solid ADC may have a better prognosis than diffuse ADC
+ Prognostic Factors
- Poor prognostic factors for nasal tumors treated with radiation therapy:
10 years (MST 6.8 months v 10.4 months)
- Facial deformity (MST 133 days v 402 days)
- Regional lymph node or pulmonary metastasis (MST 109 days v 393 days)
- Modified tumor stage II (MST 7.0 months v 17.2 months)
- Radiation therapy not included in the treatment protocol (MST 126 days v 424 days)
- Radiation total dose > 55 Gy (MST 7.1 months v 10.1 months)
- Lack of resolution of clinical signs after radiation therapy (MST 133 days v 476 days)
+ Type of Radiation Therapy
- Megavoltage radiation therapy is preferred for the treatment of nasal tumors in dogs
- Cobalt radiation therapy is associated with a significantly worse outcome compared to orthovoltage radiation therapy (MST 7.6 months v 18.0 months)
NASAL CAVITY TUMORS
| I | Ipsilateral tumor with no or minimal bone destruction | II | Bilateral tumor with moderate bone destruction | III | Bilateral tumor with extranasal extension |
| I | Ipsilateral tumor with no or minimal bone destruction | II | Bilateral tumor with moderate bone destruction | III | Bilateral tumor with extranasal extension |
| Authors | Radiation Type | MST | 1-Year Surv Rate | 2-Year Surv Rate | Thrall & Harvey, JAVMA, 1983 | Orthovoltage | 23 months | 57% | 48% | Adams et al, JAVMA, 1987 | Orthovoltage | 8.1 months | - | - | Evans et al, JAVMA, 1989 | Orthovoltage | 16.5 months | 54% | 43% | Northrup et al, JVIM, 2001 | Orthovoltage | 7.4 months | 37% | 17% | Adams et al, JAVMA, 1987 | Megavoltage | 8.1 months | - | - | McEntee et al, Vet Radiol, 1991 | Megavoltage | 12.8 months | 59% | 29% | Théon et al, JAVMA, 1993 | Megavoltage | 12.6 months | 60% | 25% | Henry et al, JVIM, 1998 | Megavoltage | 14.1 months | - | - |