

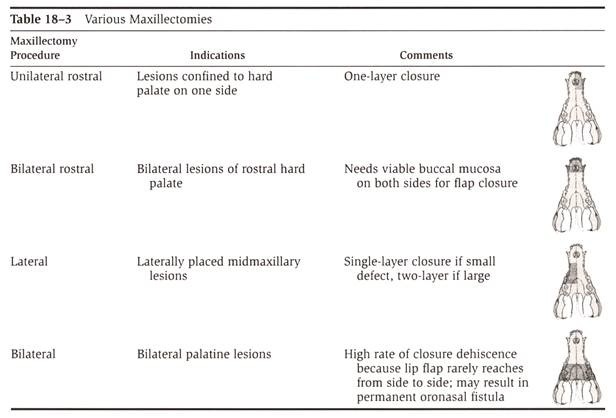
+ GENERAL CONSIDERATIONS
- Partial maxillectomy removes portions of maxilla, incisive bone, palatine bone ± portions of the zygomatic and lacrimal bones
- Premaxillectomy: unilateral or bilateral with removal of incisive bone and perhaps rostral maxilla
- Central maxillectomy: maxilla and portions of hard palate resected
- Caudal maxillectomy: maxilla, hard palate, zygomatic, and lacrimal bones removed
- Hemimaxillectomy: removal of entire maxilla on 1 side extending dorsally to ventral orbit
- Orbitectomy: removal of orbit ± caudal maxilla and vertical mandibular ramus
 From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
+ Indications
- Indications for maxillectomy include benign and malignant oral tumors, oronasal fistula along the dental arcade, and maxillary fractures
- Partial maxillectomy is limited by:
- Extension into labial or buccal tissue
- Extension across midline of central or caudal hard palate
- Sufficient skin must be available to reconstruct oronasal defect after unilateral or bilateral premaxillectomy or unilateral partial maxillectomy (i.e., labial or buccal tumor involvement)
- Antibiotics are not indicated as surgery considered dirty and risk of infection very low due to excellent blood supply
- Monofilament absorbable recommended as relatively non-reactive (minimizing mucosal irritation) and maintain adequate tensile strength
- Reverse-cutting swaged needles are preferred for suturing through tough fibrous tissue of oral cavity
- Owner satisfaction with mandibulectomy and maxillectomy procedures: 85%
UNILATERAL PREMAXILLECTOMY
+ General Considerations
- Indication: rostral maxillary tumors not crossing midline and rostral to PM2
- Tumor types: acanthomatous epulis and SCC
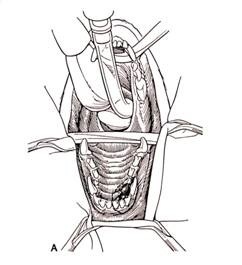
+ Surgical Technique
- Labial and gingival mucosa rostral and lateral to the mass are excised with 1 cm minimum margins
- Incision is continued through hard palate medial and caudal to lesion
- Oscillating bone saw or osteotome is used to perform osteotomies over previous mucosal incisions
- Curved bone margins will reduce tension and improve apposition and healing compared to square margins
- Resected segment of bone is removed en bloc by severing soft tissue attachments
- Hemorrhage from hard palate incision, branches of the major palatine artery, and nasal cavity is usually brisk and should be controlled with digital pressure, electrocoagulation, or ligation
- Turbinectomy should be performed if tumor invasion or iatrogenic trauma is evident

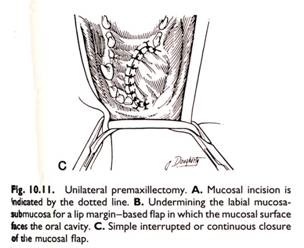
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
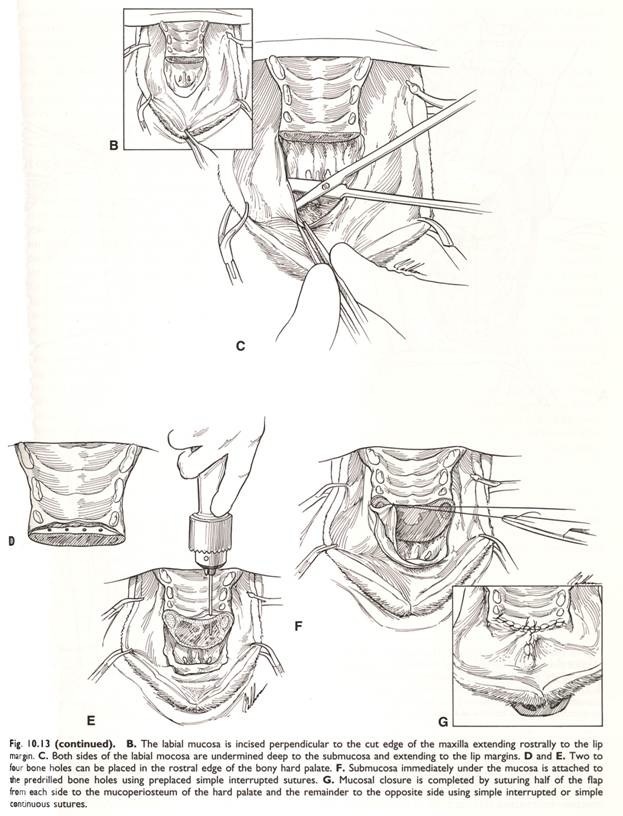
- Closure with a full-thickness labial mucosal-submucosal flap using 1- or 2-layers
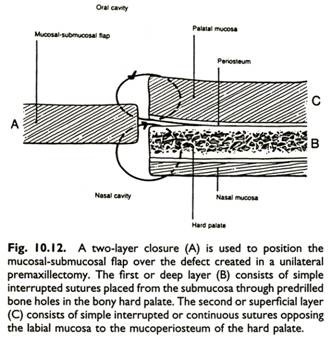
- 2-layer closure is recommended for animals receiving adjuvant chemotherapy or radiation therapy
- 2-layer closure consists of deep layer of simple interrupted sutures through predrilled holes in the bony hard palate and superficial layer apposing palatal mucosa to labial mucosa
- Palatal mucosa undermined by 2-3 mm may assist in tissue apposition
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
BILATERAL PREMAXILLECTOMY
+ General Considerations
- Indications: rostral maxillary tumors crossing midline and rostral to PM2 and has been described in combination with nasal planum resection for tumors affecting both the nasal planum and premaxilla
+ Surgical Technique for Standard Premaxillectomy
- Labial and gingival mucosa rostral and lateral to the mass are excised with 1 cm minimum margins
- Incision is continued caudally through hard palate
- Oscillating bone saw or osteotome is used to perform osteotomies over palatal incision
- Curved bone margins will reduce tension and improve apposition and healing compared to square margins
- Resected segment of bone is removed en bloc by severing soft tissue attachments
- Hemorrhage from hard palate incision, branches of the major palatine artery, and nasal cavity is usually brisk and should be controlled with digital pressure, electrocoagulation, or ligation
- Turbinectomy should be performed if tumor invasion or iatrogenic trauma is evident
- Closure with a full-thickness labial mucosal-submucosal flap using 1- or 2-layers
- 2-layer closure is recommended for animals receiving adjuvant chemotherapy or radiation therapy
- 2-layer closure consists of deep layer of simple interrupted sutures through predrilled holes in the bony hard palate and superficial layer apposing palatal mucosa to labial mucosa
- Palatal mucosa undermined by 2-3 mm may assist in tissue apposition
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
+ Surgical Technique for Combined Premaxillectomy and Nasal Planum Resection
- Premaxillectomy has been combined with nasal planum resection for rostral maxillofacial tumors
- Premaxillectomy level was initially described rostral to the maxillary canine, however, maxillectomy can be performed as far caudal as PM3 with good functional results and acceptable cosmetic appearance
- Aggressive bilateral maxillectomy techniques result in good to excellent rates of complete histologic resection and local tumor control with low rates of local tumor recurrence (0%-14%)




From: Kirpensteijn J, et al: Combined resection of the nasal planum and premaxilla in three dogs. Vet Surg 23:341-346, 1994.
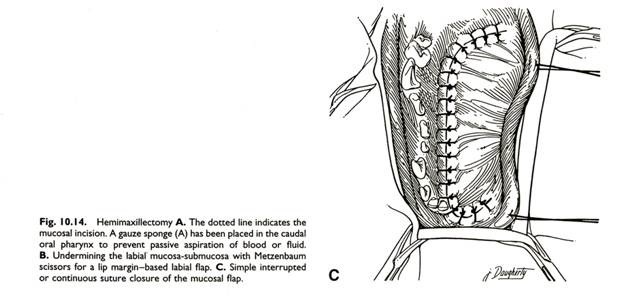
HEMIMAXILLECTOMY
+ General Considerations
- Indications: lateral maxillary tumors involving majority of hard palate and not crossing midline
- Hemimaxillectomy involves removal of oral mucosa, teeth, and segments of the incisive, maxillary, palatine, and zygomatic bones
- Extent of surgery is determined by the size of the lesion, location, degree of soft tissue involvement, and expected biologic behaviour of the tumor
- Caudal maxillectomy can be combined with resection of the inferior orbit, zygomatic arch, and vertical mandibular ramus depending on the degree of tissue involvement
- Combined dorsal and ventral approach to maxilla is recommended for large lateral or dorsal maxillary masses as bipedicled tissue flap over lateral aspect of maxilla can be retracted dorsally or ventrally to provide excellent exposure for dorsal osteotomy
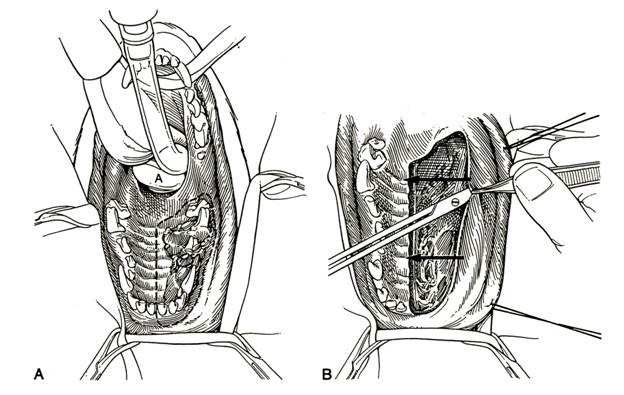
+ Intraoral Surgical Technique
- Mucosal incision started at labial-gingival margin dorsal to the middle incisors and continued laterally and caudally to the level of M2
- Medial incision started at central incisors and extended through midline of hard palate caudally to level of M2
- Mucosal and palatal incisions are joined caudally with an incision caudal to M2 at the junction of the hard and soft palate
- Terminal branches of maxillary artery (i.e., infraorbital, sphenopalatine, and minor palatine arteries) are identified and ligated at the caudal aspect of the surgical field
- Oscillating bone saw or osteotome is used to perform osteotomies over palatal incision
- Curved bone margins will reduce tension and improve apposition and healing compared to square margins
- Resected segment of bone is removed en bloc by severing soft tissue attachments
- Hemorrhage from hard palate incision, branches of the major palatine artery, and nasal cavity is usually brisk and should be controlled with digital pressure, electrocoagulation, or ligation
- Turbinectomy should be performed if tumor invasion or iatrogenic trauma is evident
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
- Closure with a full-thickness labial mucosal-submucosal flap using 1- or 2-layers
- 2-layer closure is recommended for animals receiving adjuvant chemotherapy or radiation therapy
- 2-layer closure consists of deep layer of simple interrupted sutures through predrilled holes in the bony hard palate and superficial layer apposing palatal mucosa to labial mucosa
- Palatal mucosa undermined by 2-3 mm may assist in tissue apposition
+ Combined Dorsolateral and Intraoral Surgical Technique
- Dorsal incision is made immediately lateral to the dorsal midline of the nasal cavity and continuing caudally ventral to the eye and along the zygomatic arch
- Skin incision is continued through the subcutaneous tissue, between the paired levator nasolabialis muscles, and to the bone
- Ventral aspect of the globe is separated from the dorsal zygomatic arch with blunt and sharp dissection
- Masseter muscle is dissected from the ventral aspect of the zygomatic arch with blunt and sharp dissection
- Dorsal osteotomy is prepared with subperiosteal elevation of periosteum and soft tissue from the resection site
- Intraoral approach, maxillectomy, and closure are performed as described above

+ BILATERAL CAUDAL MAXILLECTOMY
- Indications: bilateral caudal hard palate lesions
- Complications: high rate of dehiscence and possibly permanent oronasal fistula
+ ORBITECTOMY
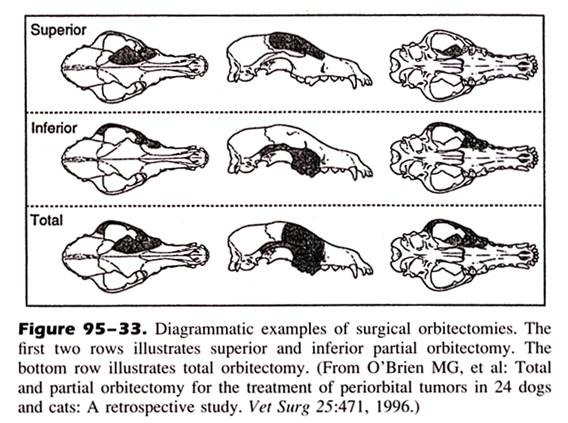
From: O'Brien MG, et al: Total and partial orbitectomy for the treatment of periorbital tumors in 24 dogs and cats: a retrospective study. Vet Surg 25:471, 1996.
POSTOPERATIVE MANAGEMENT AND RESULTS
+ General Considerations
- Sedation may be required if anxious when cannot nose breathe
- Analgesia
- Food and water offered but eating may be difficult if lip drawn into mouth
- Lip defect often resolves with tissue stretching and animal becoming accustomed to defect although occasionally chelioplasty procedures are required
- Feed soft food for 4 weeks and prevent chewing on hard objects
- Intravenous fluids continued until animal is eating and drinking enough to maintain hydration
- Self mutilation prevented with Elizabethan collar
+ Cosmetic Appearance
- Degree of facial deformity is minimal with premaxillectomy if ipsilateral canine tooth preserved
- Upper lip more medial and lower canine may protrude lateral lip if canine tooth not preserved
- Central, caudal and hemimaxillectomies will raise upper lip shortened and create concavity
- Upper lip moves with respiration for 1st 24-72 hours
- Marked deformity with resection of both upper canines in bilateral premaxillectomy
- Ventral nasal deviation corrected with dorsal nasal cartilage sutured to distal nasal bones
+ Complications
Oronasal Fistula
- Oronasal fistula due to tension, electrocautery, suture material, adjunctive chemotherapy or radiation therapy, and physical status of patient (tube feeding may be required)
- Tissue apposition important with sufficient bites to prevent suture pull-out
- Dehiscence more common when resection caudal to PM1
- Treatment: debrided and labial flap further undermined and resutured as described
Mucosal Ulceration on Labial Flap or Lateral Skin of Lip
- Trauma from the mandibular canine tooth
- Temporary problem which resolves when upper lip swelling subsides
- Mandibular canine tooth may need to be removed or be shortened with root canal procedure performed
- Damage to adjacent alveolus with tooth root damage and tooth loss
Hemorrhage
- Hemorrhage worse with caudal maxillectomy
- Hemorrhage results in anemia in 9% of partial maxillectomy cases
- Temporary unilateral or bilateral carotid artery occlusion can decrease blood loss and improve visualization as blood flow to the nasal cavity and palatal mucosa originates from the terminal branches of the external carotid artery (i.e., sphenopalatine, major and minor palatine, infraorbital, and dorsal and lateral nasal arteries)
Infection
Rare due to excellent blood supply
Sneezing and Nasal Discharge
- Respiratory noise and serosanguineous discharge common
- Cause: turbinate damage, inflammation and turbulent airflow through nasal cavity
- Violent sneezing may precipitate subcutaneous emphysema
- Chronic respiratory infections, persistent sneezing and mucopurulent nasal discharge may result if loss of defense mechanisms from extensive turbinate damage
Epiphora
- Damage to structures at medial canthus during caudal and total hemimaxillectomy
- Nasolacrimal duct is stented with monofilament non-absorbable suture material to allow epithelialization of new duct if nasolacrimal duct damage is suspected
- Other ocular damage: traumatic uveitis, hyphema, globe rupture, retinal detachment, and blindness
- Slight enophthalmos and ventral strabismus expected with ventral orbital resection
Other Complications
Prehension and mastication problems, pain, cosmetic alterations, dehiscence, infection, tumor recurrence, subcutaneous emphysema, and failure to nose breathe
Outcome
- Mandibulectomy can be curative for epulis ± SCC
- Local tumor recurrence occurs in 41%-50% dogs with complete histologic resection
- Local tumor recurrence is more common following maxillectomy compared to mandibulectomy
- Local tumor recurrence is more common for malignant melanoma, FSA, and OSA
- Outcome following maxillectomy is better for benign disease, complete histologic resection, and rostral tumors
- Dogs with incomplete histologic resection are 3.6-times more likely to have a tumor-related death
- Dogs with caudal oral maxillary tumors are 4.3-times more likely to have a tumor-related death compared to dogs with tumors rostral to the 3rd premolar
MAXILLECTOMY
| Tumor Type | Local Tumor Recurrence | Median Survival Time |
| Acanthomatous Epulis | 10% | > 26 months |
| Ameloblastoma | 13% | > 22 months |
| Malignant Melanoma | 40% | 8 months |
| Squamous Cell Carcinoma | 31% | 18 months |
| Fibrosarcoma | 46% | 12 months |
| Osteosarcoma | 35% | 5 months to > 5 years |