

+ GENERAL CONSIDERATIONS
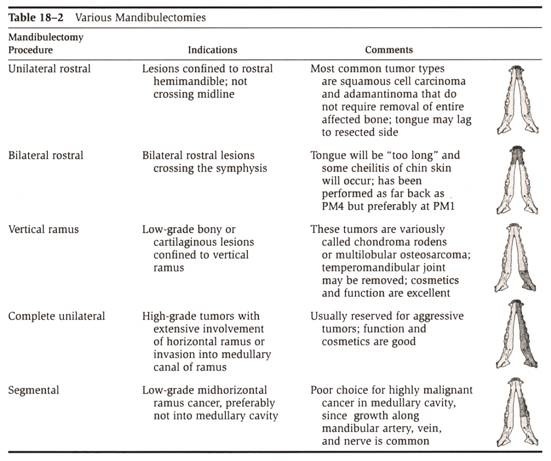
- Types of mandibulectomy: unilateral rostral, bilateral rostral, segmental, caudal, and hemimandibulectomy
- Indications: benign and malignant oral tumors involving bone or periosteum, mandibular fractures (for which primary repair is not possible or has failed), and osteomyelitis
- Antibiotics are not indicated as surgery considered dirty and risk of infection very low due to blood supply
- Monofilament absorbable is recommended as relatively non-reactive (minimizing mucosal irritation) and maintain adequate tensile strength
- Reverse-cutting swaged needles are preferred for suturing through tough fibrous tissue of oral cavity
- Analgesia with regional nerve block of inferior alveolar nerve
- Owner satisfaction with mandibulectomy and maxillectomy procedures: 85%
 From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
UNILATERAL ROSTRAL MANDIBULECTOMY
+ General Considerations
- Indication: rostral mandibular tumors not crossing midline and rostral to PM2
- Tumor types: acanthomatous epulis and SCC
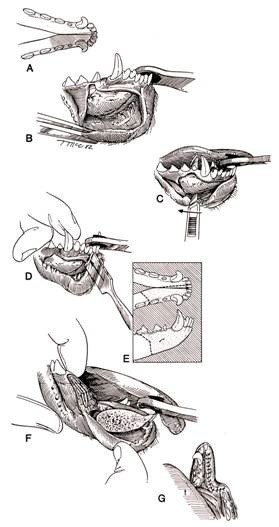
+ Surgical Technique
- Position: lateral recumbency with affected side facing dorsally
- Labial mucosa incised with 1 cm minimum margins around gross mass
- Dissection is continued around mandibular body to caudal extent of mandibular symphysis or osteotomy site
- Sublingual and mandibular salivary gland ducts open under body of tongue at sublingual caruncle and should be preserved
- Rostral osteotomy should be eccentric (i.e., between contralateral incisors or between contralateral canine and incisors) to ensure complete resection of mandibular symphysis
- Caudal osteotomy should be tapered at the occlusional margin to minimize wound tension
- Closure: mucosa with monofilament absorbable suture material in a simple interrupted or continuous pattern
 From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
+ Complications
Tongue lags to resected side
BILATERAL ROSTRAL MANDIBULECTOMY
+ General Considerations
- Indications: rostral mandibular tumors crossing midline and rostral to PM1 (± up to PM4)
- Complications: cheilitis and excessive tongue length
+ Surgical Technique
- Position: dorsal, lateral, or sternal recumbency
- Dorsal recumbency provides superior exposure for dissection and osteotomy
- Ventral recumbency provides superior exposure for more difficult wound closure
- Labial mucosa incised with 1 cm minimum margins around gross mass
- Dissection is continued around mandibular body caudally to osteotomy site
- Sublingual and mandibular salivary gland ducts should be preserved
- Mandibular body transected in caudodorsal to rostroventral direction to allow apposition of mucosa over mandible without tension
- Mandibular stabilization is not necessary (although bone screws, bone graft, or pins have been reported)
- Redundant skin may need to be removed before closure by excising V-shaped wedges rostrally or laterally
- Rostral soft tissue ridge (or dam) can help maintain saliva in mouth
- Closure: labial mucosa attached to skin to sublingual mucosa using monofilament absorbable suture material in a simple interrupted pattern
+ Complications
- Mandibular shortening
- Excessive drooling
SEGMENTAL MANDIBULECTOMY
+ General Considerations
- Indications: benign tumors and low-grade malignant tumors of the mid-horizontal mandible which do not penetrate cortical bone
- Contraindications: malignant tumors because extension along mandibular artery, vein, and nerve is common
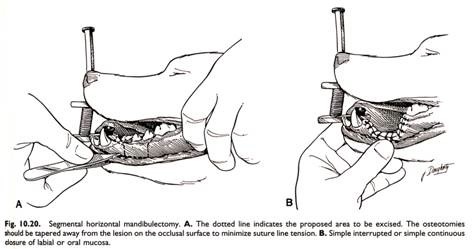
+ Surgical Technique
- Position: lateral recumbency
- Labial and lingual mucosa is incised with 1 cm minimum margins around gross tumor
- Dissection is continued around mandibular body until fully exposed
- Osteotomy performed 1 cm rostral and caudal to gross margins so that dorsal aspect angled away from mass
- Closure: labial mucosa to lingual mucosa with monofilament absorbable suture material in a simple continuous pattern
 From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
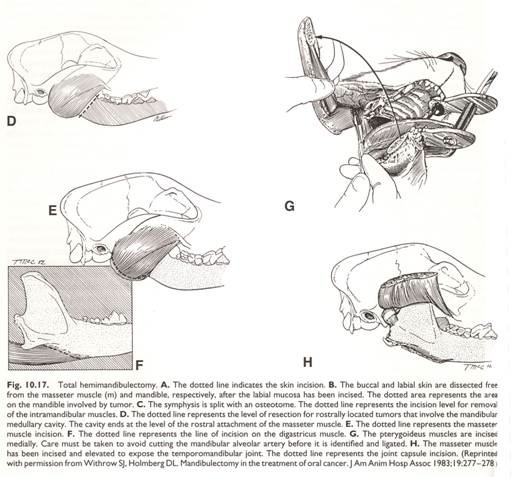
HEMIMANDIBULECTOMY
+ General Considerations
- Indications: high-grade tumors with extensive involvement of horizontal ramus or invasion into the medullary canal
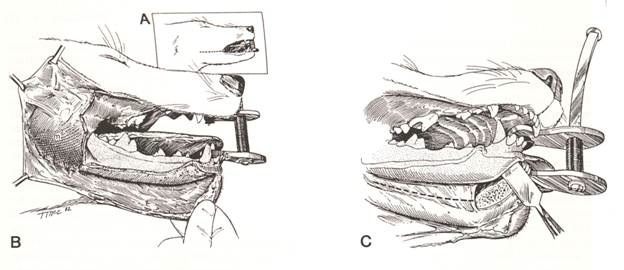
+ Surgical Technique
- Position: lateral recumbency
- Commissure of lip incised full thickness to rostral aspect of vertical ramus to improve exposure:
- Branches of facial artery and vein are ligated if encountered
- Parotid salivary duct is usually dorsal to incision
- Labial and buccal mucosa is incised with 1 cm minimum margins around the gross mass and extending caudally to the vertical ramus
- Mandibular and sublingual salivary ducts are identified and ligated
- Genioglossus, geniohyoideus, and mylohyoideus are transected from the medial aspect of the mandible
- Sublingual mucosa is incised to free the lateral border of the tongue
- Mandibular symphysis is separated to allow free lateral movement of the hemimandible and enhance exposure and visualization for caudal dissection
- Subtotal mandibulectomy can be performed at the rostral edge of masseter muscle insertion on the mandible for rostral tumors with bone marrow involvement resulting in preservation of the vertical ramus and temporomandibular joint
- Total mandibulectomy involves dissection of :
- Masseter muscle from ventrolateral surface and ventral margin of ramus with caudodorsal retraction
- Digastricus muscle from insertion on caudoventral border of horizontal mandible
- Pterygoid muscles from insertion on medial aspect of caudoventral surface of angle of mandible
- Temporomandibular joint capsule is incised laterally and medially and luxated
- Temporalis muscle from insertion on coronoid process of mandible
identification and ligation of mandibular alveolar artery and vein as it courses over the lateral surface of medial pterygoid muscle before entering mandibular foramen (ventromedial and rostral to border between angular and coronoid processes of mandible)
3-layer closure:
- Deep layer consists of opposing pterygoid, masseter and temporalis muscles
- Submucosa
- Mucosa (and skin if lip commissure incision performed)
- Monofilament absorbable suture material used in a simple continuous pattern if no tension or simple interrupted pattern if tension
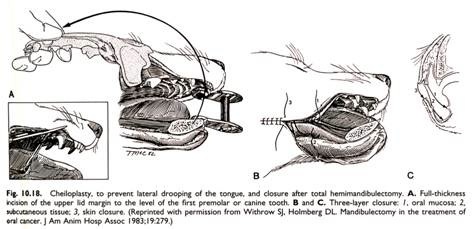
- Lip commissure can be advanced rostrally to level of canine or PM1 to prevent hanging of tongue (and a vertical mattress with a stent recommended at rostral extent due to excess tension when opening mouth)
 From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
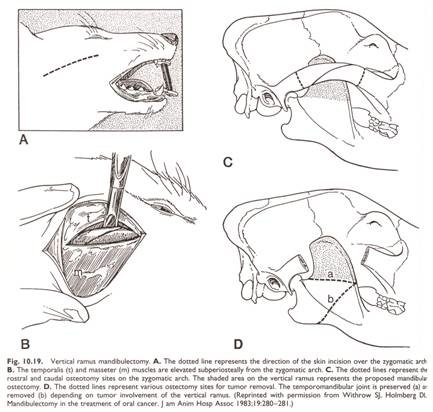
VERTICAL RAMUS MANDIBULECTOMY
+ General Considerations
- Indications: low-grade or cartilaginous lesions confined to the vertical ramus
- Vertical ramus mandibulectomy can preserve temporomandibular joint or involve excision of the mandibular ramus from M1 caudally
- Vertical ramus mandibulectomy can be combined with inferior orbitectomy for tumors with more extensive soft tissue involvement
+ Surgical Technique
- Position: lateral recumbency
- Curved skin incision performed over ventral aspect of zygomatic arch
- Temporalis muscle is subperiosteally elevated off the dorsal aspect of the zygomatic arch
- Masseter muscle is subperiosteally elevated off the medial aspect of the zygomatic arch
- Infraorbital artery, vein, and nerve course along medial aspect of zygomatic arch and should be preserved
- Zygomatic arch osteotomies performed at rostral and caudal margins with oscillating saw or Gigli wire (an osteotome tends to shatter rather than cut hard, brittle bone of the zygomatic arch)
- Masseter muscle is elevated from the ventrolateral surface and ventral margin of the ramus
- Temporalis muscle is elevated from its rostromedial insertion on the coronoid process of the mandible
- Mandibular alveolar artery and vein should be identified and preserved as it courses over the lateral surface of the medial pterygoid muscle before entering the mandibular foramen if the temporomandibular joint is preserved
- Mandibular alveolar artery and vein are ligated and transected if the temporomandibular joint is included in the mandibulectomy as the medial pterygoid muscle is elevated from the ventromedial aspect of the mandibular angle
 From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
From: Bojrab RM (ed): Clinical Techniques in Small Animal Surgery (2nd ed).
3-layer closure:
- Fascia of temporalis and masseter muscle are opposed
- Subcutaneous tissue
- Skin
POSTOPERATIVE MANAGEMENT
+ General Considerations
- Analgesia
- Feed soft food for 4 weeks and prevent chewing on hard objects
- Intravenous fluids continued until animal is eating and drinking enough to maintain hydration
- Self mutilation prevented with Elizabethan collar
+ Cosmetic Appearance
- Segmental mandibulectomy and unilateral rostral mandibulectomy: no change
- Bilateral rostral mandibulectomy causes most marked changes with shortened jaw, excessive drooling, and tongue hanging out during panting
- Total hemimandibulectomy: mild concavity, mandibular drift, and tongue hangs out
+ Complications
Swelling
Common after central, caudal, and total hemimandibulectomy with resolution in 5-7 days
Ranula
- Ranula-like lesion most often due to hematoma formation ± trauma to mandibular and sublingual salivary ducts
- Ranula-like lesions will often resolve spontaneously
Wound Dehiscence
- Wound dehiscence usually seen 3-7 days postoperatively and reported in 8%-33% cases
- Rostral end of the transected bone and lip commissure are common sites for wound dehiscence
- Dehiscence due to tension, electrocautery, suture material, adjunctive chemotherapy or radiation therapy, and physical status of patient (tube feeding may be required)
- Treatment: 2nd intention healing for small areas or debridement and suture for larger defects
- Lip commissure dehiscence treated with debridement and suturing to improve appearance
- E-tube for 1-2 weeks if tongue is the cause of tension
- Tension relieving sutures can be used such as vertical mattress
Excessive Drooling
- Excessive drooling is common and either resolves or reduces after several weeks
- Excessive drooling can cause cheilitis and facial dermatitis (especially in cats)
- Treatment: chelioplasty and daily washing for cats
Malocclusion
- Mandibular drift due to loss of mandibular support at either the symphysis or temporomandibular joint (especially in cats)
- Clinical signs: canine tooth contacts and ulcerates hard palate
- Treatment ranges from nothing to shortening or extraction of the canine tooth ± mandibular reconstruction with ulnar or rib autografts
Degenerative Joint Disease of Temporomandibular Joint
Radiographic diagnosis but rarely symptomatic
Prehension and Mastication Difficulties
- Difficulty eating in postoperative period reported in 44%
- Prehension difficulties most following bilateral rostral mandibulectomy caudal to PM2
- Mandibular drift can also result in difficulties prehending and chewing
- Hypoglossal nerve injury should be considered with prehension difficulties
- Treatment: tube feeding 1-2 weeks
Hemorrhage
- Profuse if mandibular alveolar artery not ligated before total mandibulectomy as mandibular alveolar artery retracts into medullary cavity
- Careful dissection around pterygoideus muscle and temporomandibular joint on caudomedial aspect of mandible during hemimandibulectomy as mandibular alveolar artery enters mandibular canal
- Carotid artery ligation performed if severe hemorrhage expected
- Hemorrhage controlled with Gelfoam, bone wax, topical 0.5% cocaine, or blood transfusion
Infection
- Rare due to large blood supply
- Treatment: debridement, copious lavage, remove dead space, provide drainage, and antibiotics
Outcome
- Mandibulectomy can be curative for epulis ± SCC
- Local tumor recurrence is more common for malignant melanoma and FSA
- Outcome following mandibulectomy is better for benign disease, complete histologic resection, and rostral tumors
MANDIBULECTOMY
| Tumor Type | Local Tumor Recurrence | Median Survival Time |
| Acanthomatous Epulis | 0% | > 28 months |
| Ameloblastoma | 22% | > 19 months |
| Malignant Melanoma | 13% | 8 months |
| Squamous Cell Carcinoma | 7% | 19-26 months |
| Fibrosarcoma | 34% | 11 months |
| Osteosarcoma | 5% | 7 months to > 5 years |