

+ Biologic Behaviour
- Mean age 8.5 years (range, 2-14 years)
- Sex predilection: 60%-70% male
- Sites: large intestine and mid-to-distal rectum
- Gross appearance is variable:
- Nodular (single or multiple)
- Pedunculated (mid-to-distal rectum)
- Annular constriction or obstruction (colon to mid-rectum)
- Metastatic rate is highly variable depending on the study
+ Clinical Signs
- Tenesmus, hematochezia, dyschezia, and rectal bleeding unassociated with defecation
- Other signs can include vomiting, diarrhea, and weight loss
- Hematochezia uncommon in mesenchymal tumors due to lack of mucosal involvement
- Cecal tumors often present with collapse and septic peritonitis due to perforatio
Diagnosis
+ Physical Examination
- Cachexia is common
- Abdominal mass is frequently palpable via either abdomen and rectal palpation
- Other findings include dehydration and abdominal pain
+ Laboratory Tests
Anemia and leukocytosis reported but occur less commonly than small intestinal tumors
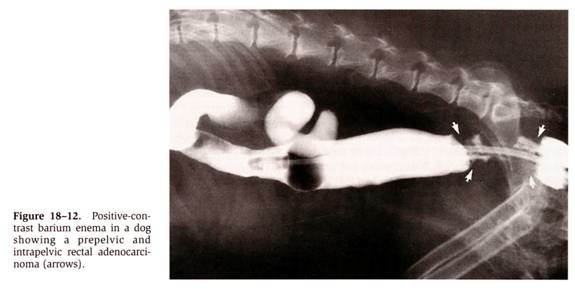
+ Contrast Radiography
- Contrast radiographs: mural lesions include luminal filling defect, intestinal wall thickening, mucosal ulceration, abnormal positioning of intestinal loops and constricting annular lesions
- Only 25% of large intestinal leiomyosarcoma required contrast studies for identification
From: Withrow SJ & MacEwen EG (eds): Small Animal Clinical Oncology (3rd ed).
+ Endoscopy
- Endoscopy is recommended prior to definitive treatment
- Biopsy samples should be interpreted histologically as cytologic misdiagnosis is common with intestinal ADC being misdiagnosed as either septic inflammation or LSA
- Biopsy samples are often small and superficial resulting in false-negative diagnosis if lesion is either submucosal or associated with surface ulceration and necrosis
+ Exploratory Celiotomy
- Definitive diagnosis with exploratory celiotomy and biopsy
- 50% of large intestinal ADC are associated with annular constrictions
TREATMENT
+ Surgery
- Debilitation and hypoproteinemia may complicate treatment
- Exploratory celiotomy with resection and end-to-end anastomosis with 4-8 cm margins and serosal patching of anastomosis
- Mesenteric and regional lymph nodes should be assessed ± aspirated
+ Chemotherapy
no effective chemotherapy for ADC
LARGE INTESTINAL ADENOCARCINOMA