

+ Biologic Behavior
- Primary rib tumors are uncommon and are usually malignant and metastatic
- OSA is the most common rib tumor in dogs and accounts for 73% of all rib tumors
- Rib OSA had a similar biologic behaviour to appendicular OSA
- Other malignant rib tumors include CSA, FSA, MCT, and HSA
- Malignant rib tumors invade the thoracic wall and can have extensive intrathoracic expansion
- 27%-45% metastatic rate for rib OSA with metastasis to the lungs very common
- Telangiectatic OSA of the rib is associated with the highest rate of metastasis
- Benign rib tumors include infiltrative lipomas and calcinosis circumscripta
+ Signalment
- No sex or breed predisposition
- Large dogs (> 20 kg) over-represented
- Median age 4.5-5.5 years for dogs with OSA and 6 years for dogs with CSA
+ Clinical Signs
- Firm and fixed thoracic wall mass
- Non-specific signs: pain, weight loss, lethargy, lameness, and dyspnea
+ Diagnosis
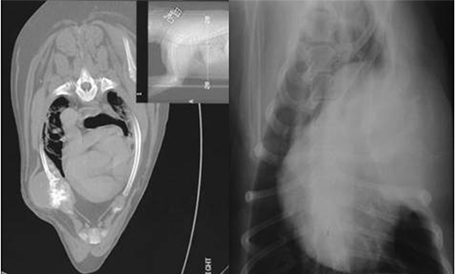
- Primary and metastatic rub tumors may produce lytic, sclerotic, or mixed radiographic patterns
- Primary rib tumors occur in the distal 3rd of rib and usually at the costochondral junction
- Radiographic features are unable differentiate OSA from CSA
- Other radiographic findings: displacement of adjacent ribs and medial displacement of parietal pleura producing extrapleural sign and displacement of intrathoracic structures such as heart and lungs
- Biopsy recommended
+ Treatment
- 3 classifications of hemipelvectomy: radical, conservative, and internal
- Radical: limb amputation with separation of pelvis through sacroiliac joint
- Conservative: limb amputation with preservation of sacroiliac joint and cranial ilium
- Internal: preservation of limb
- Musculocutaneous flaps are preferred for wound closure although fasciocutaneous flaps acceptable
- Medial extent of the tumor is the most difficult dissection with midline (sacrum or pubis) the surgical limit
- Complications are rare and similar to limb amputation
- Complications in humans include infection, skin flap necrosis, herniation, fecal and urinary incontinence if pudendal nerve roots transected, thromboembolic disease, and local tumor recurrence

+ Prognosis
- MST 120 days for OSA following chest wall resection, with 6-month survival rate 20%
- MST 240 days for OSA following chest wall resection and chemotherapy is 240 days
- MST 299-1,080 days for CSA
- Survival times range from 120-450 days for dogs with FSA
- Survival times range from 30-150 days for dogs with HSA
- Prognostic factors: tumor type and complete histologic resection
- Local tumor recurrence ± metastasis is 5.6-times more likely with incomplete resection